Let’s say the National Institutes of Health (NIH) just handed us a multi-million dollar grant to get to the bottom of TMD and find a cure once and for all. I mean, we could start handing out heating pads left and right, but that kind of relief can only get us so far. Whenever I try a different form of therapy or medication, I like to think about the biology, right down to the cellular and molecular level. Why are the cells that make up my jaw region being such jerks?
I think it’s important to have some kind of understanding of what’s going on in my body and how medications will affect me, especially for a chronic illness that can require long-term medication use. It’s also especially important in a field like TMD healthcare, with 14 different sub-specialists recommending 14 different treatments.
To guide our thought experiment, we’ll be using the paper Pharmacotherapy in Temporomandibular Disorders: A Review by Ouanounou and colleagues (2017). This review paper1 explores seven major categories of the most commonly prescribed medications for TMD pain and examines the literature on how these drugs work, if they work, and the evidence to back it up.
The Science
Before sinking our teeth in, probably the first place to start to identify a TMD cure is to consider the biology. TMD (also referred to as TMJ) stands for temporomandibular joint disorder, which isn’t exactly a neat, simple diagnosis. Rather, it’s an umbrella term that encompasses a number of different etiologies (causes) and symptoms. The temporomandibular joint itself is part of the underlying etiology in some—but not all—cases, but most chronic TMD patients experience some kind of pain in their facial or jaw muscles. We experience pain only because our nerves send a signal to the brain, instructing it to make us feel pain (thanks a lot). For that reason, a significant number of TMD medications affect our neurons and nervous tissue.
Now why do our neurons send these pain messages to the brain? So first, a philosophical or evolutionary perspective. Why the heck would we spend billions of years evolving only to cower in pain from a measly hot coal or the pinch of a bee sting? In reality, it’s not the pain that kills us. The pain is the smoke alarm. It’s the lighthouse off the rocky pier. It’s just the thought of having to go to the DMV (…kidding). People born without pain receptors, whose alert systems are broken, tend to die in childhood because feeling physical pain that alerts us to dangerous situations—like being on fire—is critical to human life. Pain confers an evolutionary advantage…but sometimes it goes haywire.
Now, biologically what causes neurons to transmit pain signals to our brain? Well, sometimes the nerves themselves may be damaged, but often the neurons are just the messenger detecting a “painful” stimulus in our joints or muscles and keeping the brain informed (again…thanks a lot). What that painful stimulus is we don’t always know: could it be muscle tension, inflammation, lactic acid buildup from active jaw muscles, neurotransmitter abnormalities… all of the above?
A common variable for many patients is tension in the jaw muscles. These muscles contract when they receive a signal from a motor neuron in the form of neurotransmitters. Essentially, here is what happens:
- A neuron connects, or synapses, onto a muscle cell.
- The neuron becomes excited, meaning it prepares to send a signal to the muscle cell.
- There is a small gap between the neuron and the muscle cell called the synapse. The excited neuron sends truckloads of neurotransmitters across the synapse to the muscle cell, instructing it to contract.
- Once the muscle cell receives this signal, it initiates contraction, or shortening – just like we need the masseter muscle to contract and shorten to close our jaw while chewing food.
- Conversely, once the signal fades away, the muscle cell relaxes, or lengthens.
In TMD, the muscles of the jaw and face are often overactive, contracting to the point of pain. As a result, these muscles enlarge over time, resulting in stronger contractions and greater pain. It used to be thought that the buildup of lactic acid, a waste product of highly active muscles, is responsible for activating pain receptors that cause muscle soreness, though this has become controversial and has been contested more recently. Another line of thought is that damage to the muscles and joints from excessive muscle contraction results in inflammation in response to cellular debris. Thus, immune cells infiltrate the area and produce inflammatory chemicals—prostaglandins, bradykinin, and substance P—that elicit pain by acting on pain receptors. These are responsible for the five cardinal signs of inflammation we’re all too familiar with: rubor (redness), calor (warmth), tumor (swelling), dolor (pain), and function laesa (loss of function) – the last one doesn’t carry the same rhetorical symmetry, but the TMD patient knows too well the frustration of loss of function.
Now armed with science, we’re left with a few options to mitigate the symptoms caused by overactive, tight muscles implicated in TMD pain. One of these targets is the inflammatory response.
Non-Steroidal Anti-Inflammatory Drugs (NSAIDs)
Nearly all of us are familiar with the pain-relieving effects of NSAIDs, from aspirin to ibuprofen. It turns out that NSAIDs are the most commonly prescribed medication for TMD pain.
Examples: aspirin, celecoxib (Celebrex), diclofenac (Voltaren), ibuprofen (Motrin, Advil), naproxen (Aleve)
Mechanism of Action: NSAIDs work by blocking inflammatory pathways. Specifically, they inhibit cyclooxygenase (COX) enzymes and thus block the production of prostaglandins, which are molecules that signal pain.
Efficacy: Evidence suggests NSAIDs may help with acute, localized TMJ inflammation,3 but they might not be much better than placebo in chronic TMD pain.4
Drawbacks: Though many are available over the counter without a prescription, NSAIDs are generally not recommended for long-term use as they can cause gastric ulcers (which is to be taken seriously, as up to 16,000 people die each year from NSAID-related GI complications!). NSAIDs can also adversely affect kidney function and blood clotting. Some medications may also interact with NSAIDs, including lithium, methotrexate, ACE inhibitors, and loop diuretics.
Corticosteroids
If NSAIDs are the rubber mallet among anti-inflammatories, corticosteroids are the sledgehammer. Corticosteroids are essentially really powerful anti-inflammatory medications, which means they typically work better than NSAIDs, but they come with greater risks.
Examples: prednisone, dexamethasone
Mechanism of Action: Like NSAIDs, corticosteroids reduce inflammation by inhibiting prostaglandin formation, though via a different target.
Efficacy: There is good evidence that corticosteroids can help with TMD pain over a period of 4–6 weeks,5 but…
Drawbacks: …there are some significant side effects. Corticosteroids are produced naturally in the adrenal glands, but high levels of synthetic corticosteroids can backfire, increasing the risk for adrenal damage, hypertension (high blood pressure), electrolyte abnormalities, diminished bone resorption, soft tissue atrophy (degeneration), and impaired immune defenses. As you can imagine, corticosteroids are rarely the first line of defense for chronic TMD pain, and even then only prescribed for short-term use.
Opioids
Anyone who has ever undergone any kind of surgery is in little doubt about the relief opioids can provide from pain. However, there are real concerns about the potential for developing tolerance and dependence, as well as questions about their long-term efficacy in chronic pain.
Examples: codeine, oxycontin (Percoset), hydromorphone (Dilaudid), fentanyl (Duragesic)
Mechanism of Action: Synthetic opioids mimic the actions of endogenous opioids our body naturally produces, such as endorphins. Opioids relieve pain by acting on opioid receptors in the nervous system, quieting neurons that would otherwise cause you to feel pain.
Efficacy: The good news is that opioids are fairly potent pain relievers.6 The bad news is that the nervous system learns and adapts to elevated opioid levels by becoming less responsive. For example, opioid receptors might become desensitized, requiring more opioids than before to achieve the same level of pain relief. Thus, opioids can alleviate TMD pain in the short-term, but one might develop tolerance or even chemical dependence in the long-term, rendering opioid therapy much less effective.
Drawbacks: Opioids are associated with some side effects (constipation, nausea, dizziness, etc.), and they can also cause and exacerbate sedation from central nervous system depressants, such as alcohol or benzodiazepines.
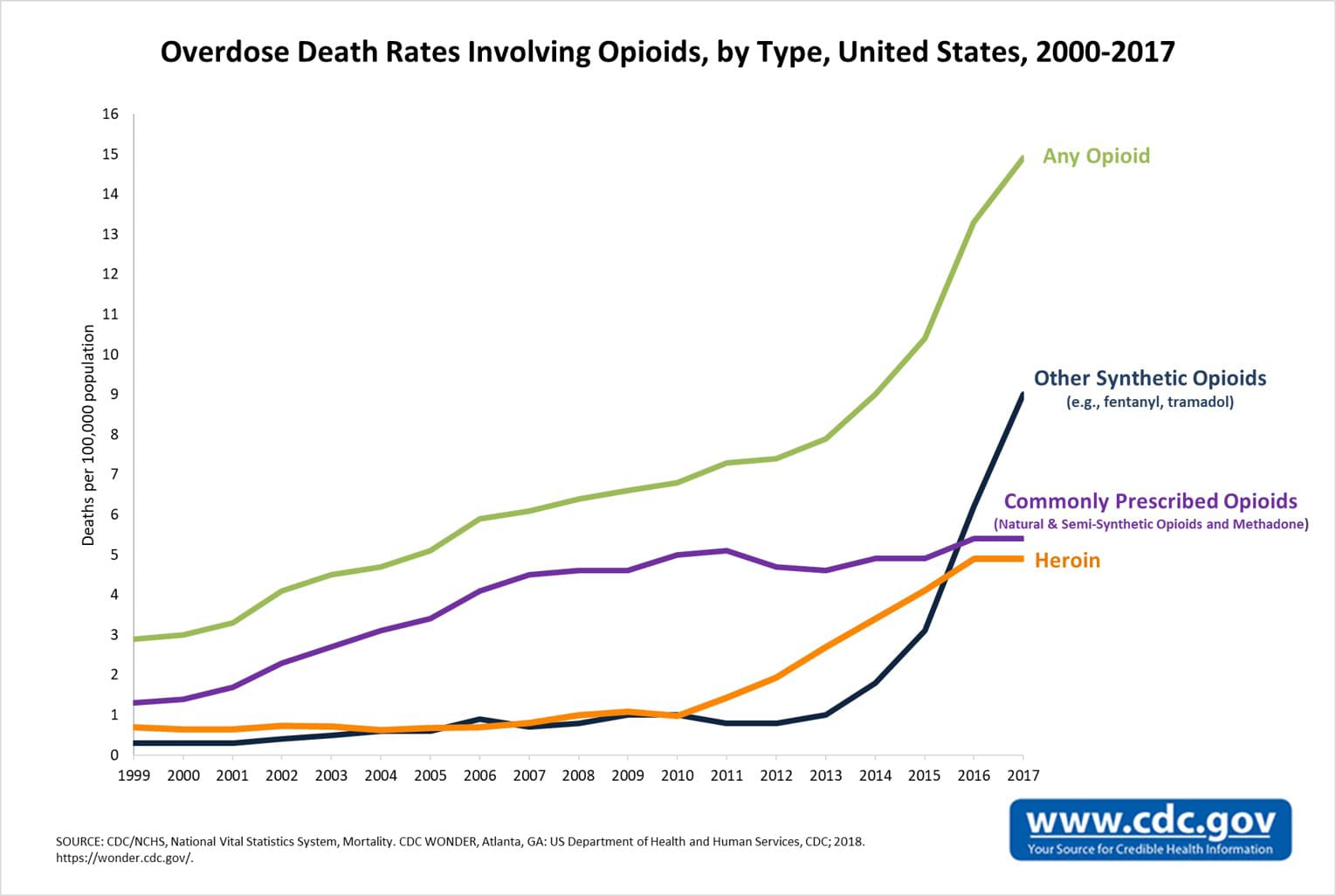
However, the main clinical concern with opioid treatment is the potential for addiction, and I would be doing a disservice to this paper, and to you, if we didn’t acknowledge the elephant in the room: the national opioid epidemic. Here are some pretty morbid stats:
- 115 people die every day in the U.S. from an opioid overdose7
- Opioid overdose deaths have ballooned nearly 4-fold in 15 years, from 8,407 deaths in 2000 to 33,091 deaths in 2015 (68% of which were from prescription opioids)8
- In 2016, more people died from opioids than died from car accidents, guns, or breast cancer9
I can see how easy it would be for someone without chronic pain to dismiss opioid therapy as a failure or to decidedly park themselves in the “anti-opioid” camp. But there don’t have to be two camps. Clearly many people do find the relief they need in prescription opioids and have found themselves on the wrong side of tightening opioid restrictions. But if anything, this crisis is a siren call for the need for more targeted therapies for TMD and other chronic pain conditions, or at least safe and effective pain-killers. For these reasons, opioid treatment is strictly monitored and regulated, and we’ll likely see more attention (and hopefully funding!) diverted towards this public health issue in the coming years.
Muscle Relaxants
Much of the pain TMD sufferers experience is thought to be caused by tight, overactive muscles in the jaw and face. So it makes sense to go straight to the source and persuade those muscles to relax, right?
Examples: cyclobenzaprine (Flexeril), carisoprodol (Soma), metaxalone (Skelaxin), methocarbamol (Robaxin), orphenadrine (Norflex), tizanidine (Zanaflex)
Mechanism of Action: Recall that muscles don’t contract on their own; they require input from the nervous system! Most muscle relaxants act not on muscle itself, but rather on the neurons that instruct muscles to contract. For example, cyclobenzaprine—the most commonly prescribed muscle relaxant for TMD pain—affects levels of the neurotransmitter norepinephrine in the brain, inhibiting the neurons that stimulate muscle contraction.
Efficacy: The jury is out on muscle relaxants. Some studies show muscle relaxants relieving muscle spasms in cervical and lumbar pain,10,11,12 but more research is needed to elucidate the direct effects of muscle relaxants on muscle-related TMD pain. On a positive note, the sedative effect of muscle relaxants can improve sleep.
Drawbacks: The primary side effect with muscle relaxants is drowsiness, so it’s recommended that muscle relaxants be taken before bedtime and not before driving. Muscle relaxants can also interact with MAOIs (monoamine oxidase inhibitors, a class of antidepressants) and tramadol (an opioid) , and they should not be taken in patients with hyperthyroidism, congestive heart failure, or other heart conditions.
Antidepressants
Science would be nowhere without serendipitous discoveries. The first antidepressant was designed as a tuberculosis drug but, by accident, was also found to alleviate depression. Similarly, some antidepressants have been found to relieve pain independently of their mood-boosting effects. Psychoactive drugs are rarely specific, so it’s unsurprising that some antidepressants are also effective analgesics. Some of these have shown promise as pain relievers for TMD pain.
Examples: tricyclic antidepressants (TCAs; amitriptyline, nortriptyline, desipramine), selective serotonin reuptake inhibitors (SSRIs; citalopram, paroxetine, fluoxetine)
Mechanism of Action: There isn’t one single mechanism of action all antidepressants use to alleviate TMD pain, and to be perfectly honest, no one knows for certain exactly how they provide pain relief. TCAs might alleviate pain by preventing the neurotransmitters norepinephrine and serotonin from being swept out of the synapse and back into the neuron, thus prolonging the amount of time those pain-relieving neurotransmitters spend activating their receptors at the synapse. It’s thought that this mechanism occurs in the spinal cord to block the transmission of pain signals. Similarly, SSRIs prevent serotonin from being swept out of the synapse, elevating serotonin levels and prolonging its effects in the synapse, and thus TCAs and SSRIs may act via a similar mechanism.
Efficacy: TCAs have been shown to be most effective for those with chronic pain, including TMD pain,13 although some conflicting findings suggest they may not be much better than placebo.14 SSRIs have been shown to alleviate neuropathic, facial, and TMD pain.15,16 Plus, the antidepressant qualities of TCAs and SSRIs are an added benefit for those with comorbid depression, although the dosages of these medications for TMD are typically much lower than when used primarily as an antidepressant. The sedative effect of TCAs may also improve sleep.
Drawbacks: Though potentially effective, TCAs carry some side effects, including constipation, dizziness, and sedation. TCAs also interact with MAOIs and are contraindicated for cardiac and elderly patients. SSRIs are safer but can cause some side effects, such as nausea, vomiting, and sexual dysfunction.
Anticonvulsants
Anticonvulsants do more than provide relief to patients with epilepsy. Since they work by quieting overactive neurons implicated in seizures, it makes sense that they might also quiet overactive neurons involved in pain signaling.
Examples: gabapentin (Neurontin), pregabalin (Lyrica)
Mechanism: Gabapentin and pregabalin structurally mimic the neurotransmitter GABA, which has an inhibitory effect on neurons. However, anticonvulsants are thought not to act on GABA receptors but rather on ion channels to inhibit neurons involved in pain transmission.
Efficacy: Anticonvulsants are often used for neuropathic pain caused by nerve damage, such as trigeminal neuralgia or diabetic neuropathy. Gabapentin has been shown to reduce TMD pain,17 but there is limited evidence that pregabalin does.
Drawbacks: Gabapentin and pregabalin are associated with some adverse effects (dizziness, blurred vision, drowsiness, etc.) but otherwise are generally considered safe.
Benzodiazepines
Not only are antidepressants used for TMD pain, but so are benzodiazepines, a class of anti-anxiety medications. Like TCAs and SSRIs, benzodiazepines may reduce TMD pain directly as well as indirectly as a result of its anti-anxiety properties.
Examples: diazepam (Valium), clonazepam (Klonopin)
Mechanism: Benzodiazepines act on benzodiazepine receptors, which are part of the inhibitory GABA receptor complex, thus blocking neuronal excitation. This mechanism is thought to explain the ability of benzodiazepines to relax acute muscle spasms, promote sleep, reduce anxiety, and even prevent seizures.
Efficacy: Evidence from multiple studies indicates that benzodiazepines can be helpful for chronic TMD pain.18,19 Furthermore, benzodiazepines can improve sleep and suppress feelings of anxiety, which may partially explain the pain relief experienced by TMD patients.
Drawbacks: Although this treatment has shown promise, the most serious risk is the potential to develop tolerance and physical dependence to benzodiazepines. Additionally, there may be some side effects (drowsiness, confusion, amnesia, etc.), and benzodiazepines interact with some medications and foods, as they affect an important liver enzyme. These medications are also contraindicated for myasthenia gravis, allergies, and acute glaucoma.
TL;DR
Here’s the final scoop on the pharmacological options for TMD relief:
Medication | Mechanism | Efficacy | Drawbacks |
|---|---|---|---|
NSAIDs (aspirin, ibuprofen) | Anti-inflammatory | May help with acute, localized pain | GI and kidney complications, some interactions |
Corticosteroids (prednisone, dexamethasone) | Anti-inflammatory | Alleviates TMD pain over 4–6 weeks | Significant side effects, not recommended long-term |
Opioids (codeine, oxycodone) | Analgesic, mimics endogenous opioids | Powerful analgesic effects in short-term | Potential for tolerance and dependence |
Muscle Relaxants (carisoprodol, cyclobenzaprine) | Muscle relaxant via central nervous system | Conflicting findings but may improve sleep | Sedative side effect but generally safe |
Antidepressants (amitriptyline, citalopram) | Analgesic, inhibits pain signals | May help with chronic TMD pain, improves sleep and comorbid depression | Sedative effect but generally safe |
Anticonvulsants (gabapentin, pregabalin) | Analgesic, inhibits pain signals | Helps with neuropathy, may help with TMD pain | Some side effects but generally safe |
Benzodiazepines (diazepam, clonazepam) | Muscle relaxant via central nervous system | Helps with TMD pain, improves sleep and comorbid anxiety | Potential for tolerance and dependence |
Despite a “wealth of analgesic options,” no miracle drug has appeared on the market yet. One of the reasons is that the efficacy of many of these options has been contested, or not quite proven.1 Some TMD patients respond well to NSAIDs, while others obtain relief from muscle relaxants or anti-anxiety medications. However, anecdotal evidence doesn’t quite cut it when applying findings to the general population. It’s not that someone’s pain relief isn’t necessarily “real,” but rather we need to better understand why a particular therapy helps select patients and not others. To be honest, this review article left me feeling a bit disappointed–sort of like a cliffhanger at the end of a movie—wishing that we had better answers to these questions.
Furthermore, the pain medications with strong track records tend to come with trade-offs, including life-threatening GI complications or the potential for tolerance and addiction. The serious risks associated with long-term NSAID, benzodiazepine, or opioid use stress the importance of pain management competency among primary care physicians, who can help their patients understand the risks and benefits of the long-term use of any of these medications, and carefully titrate them to the level that provides sufficient pain relief at the least risk.
One of the major takeaways from this review is that there is a deficiency of well-designed randomized controlled trials, particularly those that that differentiate by TMD etiology and symptoms to identify who is most likely to be helped by a given treatment. If the NIH handed us a multi-million dollar grant, the first place to start would be to take some of these promising contenders and conduct rigorous randomized controlled trials with large sample sizes, longitudinal follow-up, and differentiation by type of TMD pain. Then, the medications that have shown therapeutic promise should be studied at a molecular level to help us understand their precise mechanisms of action. If there is money to spare—or the NIH extends us another grant thanks to all our efforts to revolutionize TMD medicine—we should work to exploit the therapeutic advantages of the medications that work while finding ways to mitigate their risks.
Sources
1 Ouanounou A, Goldberg M, Haas DA. Pharmacotherapy in Temporomandibular Disorders: A Review. J Can Dent Assoc 2017;83:h7
2 Image adapted from OpenStax under CC BY 3.0: https://cnx.org/contents/bfiqsxdB@3/Skeletal-Muscle
3 Ta LE, Dionne RA. Treatment of painful temporomandibular joints with a cyclooxygenase-2 inhibitor: a randomized placebo-controlled comparison of celecoxib to naproxen. Pain. 2004;111(1-2):13-21.
4 Wright EF. Manual of temporomandibular disorders. 2nd ed. Ames, Ia.: Wiley-Blackwell; 2010.
5 Alstergren P, Appelgren A, Appelgren B, Kopp S, Lundeberg T, Theodorsson E. The effect on joint fluid concentration of neuropeptide Y by intra-articular injection of glucocorticoid in temporomandibular joint arthritis. Acta Odontol Scand. 1996;54.
6 Haas, DA. An update on analgesics for the management of acute postoperative dental pain. J Can Dent Assoc. 2002.68(8):476-82.
7 CDC/NCHS, National Vital Statistics System, Mortality. CDC Wonder, Atlanta, GA: US Department of Health and Human Services, CDC; 2017. https://wonder.cdc.gov.
{kind=link}
8 National Institute on Drug Abuse. “Overdose Death Rates.” NIDA, 15 Sept. 2017, www.drugabuse.gov/related-topics/trends-statistics/overdose-death-rates.
9 Nydailynews. “Opioid Overdoses Kill More People in U.S. than Guns or Breast Cancer.” Nydailynews.com, 21 Dec. 2017, beta.nydailynews.com/news/national/opioid-overdoses-kill-people-u-s-car-accidents-article-1.3713354.
10 Hersh EC, Balasubramaniam R, Pinto A. Pharmacologic management of temporomandibular disorders. Oral Maxillofac Surg Clin N Am. 2008;20(2):197-210.
11 Brown BR Jr, Womble J. Cyclobenzaprine in intractable pain syndromes with muscle spasm. JAMA. 1978;240(11):1151–2.
12 Borenstein DG, Korn S. Efficacy of a low-dose regimen of cyclobenzaprine hydrochloride in acute skeletal muscle spasm: results of two placebo-controlled trials. Clin Ther. 2003;25(4):1056-73.
13 Rizzatti-Barbosa CM, Nogueira MT, de Andrade ED, Ambrosano GM, de Barbosa JR. Clinical evaluation of amitriptyline for the control of chronic pain caused by temporomandibular joint disorders. Cranio. 2003;21(3):221-5.14 McQuay and Moore, 1997
15 Lee YC, Chen PP. A review of SSRIs and SNRIs in neuropathic pain. Expert Opin Pharmacother. 2010;11(17):2813-25.
16 Sindrup SH, Gram LF, Brøsen K, Eshøj O, Mogensen EF. The selective serotonin reuptake inhibitor paroxetine is effective in the treatment of diabetic neuropathy symptoms. Pain. 1990;42(2):135-44.
17 Berry JD, Petersen KL. A single dose of gabapentin reduces acute pain and allodynia in patients with herpes zoster. Neurology. 2005;65(3):444-7.
18 Singer E, Dionne R. A controlled evaluation of ibuprofen and diazepam for chronic orofacial muscle pain. J Orofac Pain. 1997;11(2):139-46.
19 Guaiana G, Barbui C. Discontinuing benzodiazepines: best practices. Epidemiol Psychiatr Sci. 2016;25(3):214-6.